
Fundable frontiers in medical research: Spatial omics.
The details we have been missing

Publications are not the currency of medical research, techniques are.
Arguably, one of the biggest medical research frontiers is spatial omics. It seems that you can browse an issue of Nature these days without running across a spatial omics paper.
In this article, I am going to show you why I think:
Spatial transcriptomics is part of a bigger frontier.
It is not just a trend but rather a new frontier in medical research that will have substantial impact.
How to incorporate it into new projects and funding proposals.
Spatial transcriptomics brings disease subclassification to a new level
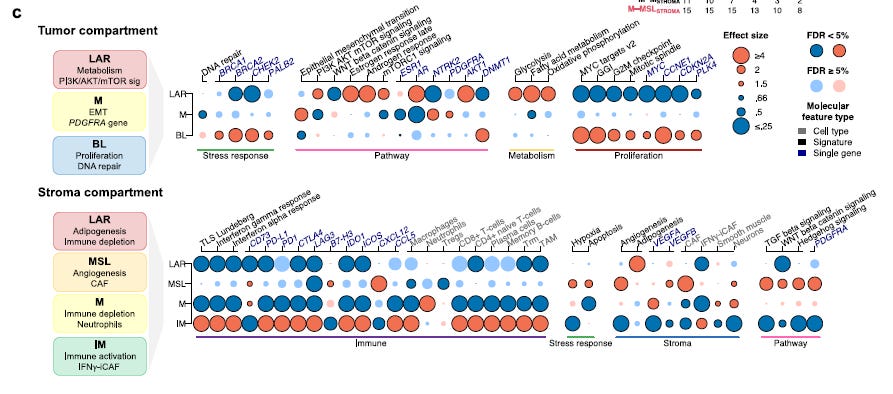
from Wang et. (1) Fig 4 Spatial deconvolution of TNBC molecular subtypes
In triple-negative breast cancer, spatial transcriptomics reveals a large degree of heterogeneity which can be used to subclassify breast cancer tumors and potentially direct therapy.
Wang et al. (1) developed a gene expression signature in triple negative breast cancer samples using spatial transcriptomics. They found a large degree of heterogeneity. This heterogeneity was then used to subclassify patients with triple negative breast cancer and the subclassification had both prognostic and predictive value for response to immunotherapies.
“This spatial deconvolution allowed us to show that tumor and stroma compartments have different contributions to TNBC molecular classification, with potential clinical implications.”
This research shows potential to get even more fine-grained on targeting therapies and finding explanations for the lack of response to therapy in subpopulations.
It gives us a glimpse of the future where we can look to different spatial dimensions to help tailor therapy.
Spatial proteomics is better at dissecting mechanisms.
Eric Topol is the Founder and Director, Scripps Research Translational Institute. He has a great newsletter, Ground Truths . In one of his recent editions (2), he reports on a landmark paper where researchers used spatial transcriptomics to identify a mechanism that was previously obscured by the loss of spatial information when bulk omics were done on samples.
Leveraging imaging, transcriptomics and AI, the researchers were able to identify in patients with Stevens Johnson syndrome that the JAK/STAT pathway was involved in causing the disease. The increased resolution of spatial proteomics revealed a mechanism that was previously obscured. Lumping cells together without regards to their spatial relationships is like trying to pick out who has a good singing voice in a stadium-wide sing-along.

from Nordmann 2024 (3) Fig. 4 The JAK/STAT pathway is potently activated in TEN.
After confirmation in laboratory models, they proceeded to treating the patients with existing treatments that targeted the pathway with dramatic results.
Topol points out that to arrive at what he calls spatial medicine, there remain multiple analytical challenges that require the use of machine learning and AI to be overcome. He further elaborates that this coincides with an increasing interest in spatial intelligence. I’d say this is a fortuitous convergence of technology frontiers.
Beyond providing mechanistic insights on the fundamental role of the JAK/STAT pathway and key cell types, a major feat on its own, showing that the insights gained from spatial omics led to effective therapy already demonstrates unmistakable impact of this frontier (3).
Why are these two papers and Topol's perspective important?
Both illustrate how spatial omics provides another unit of analysis in our bid to better subclassify disease. It makes perfect sense that the different dimensions need to be considered. The human body is spatially heterogeneous.
The more and more detail we can take into a conceptualization of disease, the better we will be able to target therapy to the right patient populations. In other words, realizing what has until now been a somewhat empty promise: the right medicine, to the right patient, at the right time.
How many more layers of detail do we need to get to, in order to fulfill that promise?
For starters, the dynamics of molecular markers over time is an aspect that is scarcely considered. Environmental factors are also just beginning to come into focus. We are just beginning to enter the spatial medicine or dimensional medicine frontier.
This the Hubble telescope of medicine.
How to build these concepts into future funding proposals?
I see three ways to include dimensional medicine into future funding proposals:
Any effort to subclassify patients should include spatial or multi-dimensional methods.
The analysis of this data is complex, so new funding to develop new techniques is relevant.
Use dimensional characterizations to improve models, both preclinical and computational.
Want to continue to learn about about fundable frontiers in medical research:
References
1. Wang, X., Venet, D., Lifrange, F. _et al._ Spatial transcriptomics reveals substantial heterogeneity in triple-negative breast cancer with potential clinical implications. Nat Commun 15, 10232 (2024). [https://doi.org/10.1038/s41467-024-54145-w](https://doi.org/10.1038/s41467-024-54145-w)
2. [https://erictopol.substack.com/p/the-dawn-of-spatial-medicine](https://erictopol.substack.com/p/the-dawn-of-spatial-medicine)
3. Nordmann, T.M., Anderton, H., Hasegawa, A. et al. Spatial proteomics identifies JAKi as treatment for a lethal skin disease. Nature 635, 1001–1009 (2024). [https://doi.org/10.1038/s41586-024-08061-0](https://doi.org/10.1038/s41586-024-08061-0)